

Medicine packer bottles pharmaceutical grade
Medicine packer bottles pharmaceutical grade
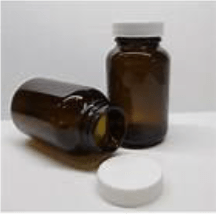
In the early 70s when I started my career in Squibb, BD, it was “Aluminum-foil Strip packaging”, putting a single unit tablet/capsule within a pocket created between two polymer laminated aluminum foil passing through two heated knurled rollers with circular/elliptical cavities/sockets drawing the tablet/capsule from the hopper through a chute by a strip packaging machine with regulated temperature melting the polymer at the knurling area of the roller to seal the strip for the each individual unit of the dosage. A cutting knife was employed to cut the strip based on required number of units of dosage. An in-process test was done for the sealing check by performing a leak-test in a beaker/device with

water, and putting one of such sealed strip with tablets/capsules and exerting vacuum. If there would be some leakage in the one of the pocket or many pockets of the strip (mostly at the beginning of the operation) air bubbles will come. Then after thoroughly wiping this strip undergone for the leakage test with towel or dry tissue, the strip was opened carefully to find which pocket tablet/capsule had actual wetness. This procedure was employed for both initial setting of the machine as well as an in-process test for the packaging process.
In mid-80s when I went to Sweden for training at the then ASTRA at Sodertalje, Sweden, to take the position of Head of the Process Technique for their newly built pharmaceutical plant in the M.E; it was pre-pocket formed “Blister” packaging. Now it was initial or simultaneous pockets created in a hard see-through polymer either colourless or with yellowish or reddish colour required to protect against light. Individual unit tablet/capsule is put inside the pre-formed pocket and then closing and sealing mostly with a thin aluminum foil laminated with polymer, by either a single unit strips packaging or continuous striping packaging machine. Initial testing and in-process testing were somewhat similar to that of aluminum foil strip packaging.

The user or the patient would open only one unit dosage from any of this system of packaging for intake. Hence, both of these above systems/procedures of packaging will not only provide protection against product stability towards its shelf-life but also any pilferage, contamination and/or physical manipulation for any ill-motive.

Pharma HDPE CRC bottle (US)

Prescription pharmacy CRC vials-Amber (US)
For such studies the college of pharmacy pharmaceutics with the collaboration of the agency (FDA) can do by simulating the conditions such as:
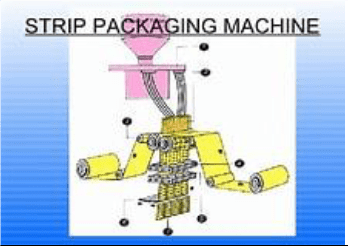
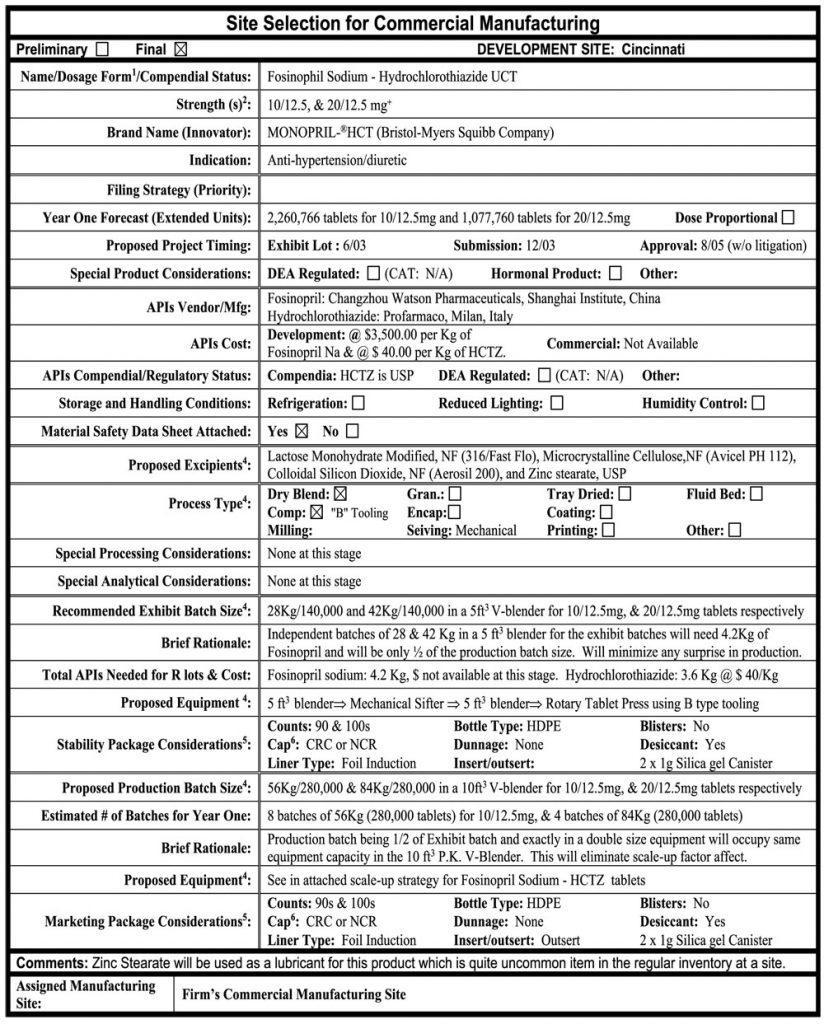
I. For the pharmacy condition: Simulating the opening of the bulk container where it is supplied in an induction sealed high density polyethylene (HDPE) bottle in bulks (1000s); for the worst scenario for 30 units DP (Tablet or capsule) dosage X number of such numbers of opening and closing simulating in that prevailing environmental condition of the pharmacy dispensing area (temperature and humidity). Do all analytics including, assay, dissolution and impurity to find if the last dosage has maintained these quality integrity.
 II. For the at actual patient use stage: Simulating the opening of the dispensed container where it is supplied in an Prescription Pharmacy CRC Vials-Amber in 30s or 90s for one month or three months supplies; for the worst scenario for 90 units DP (Tablet or capsule) dosage X number of such numbers of opening and closing simulating in that prevailing environmental condition at home in a medicine cabinet most likely within the vicinity of the bath-room where there is possibility of high-humidity and in winter temperature conditions. Do all analytics including, assay, dissolution and impurity to find if the last dosage has maintained these quality integrity.
II. For the at actual patient use stage: Simulating the opening of the dispensed container where it is supplied in an Prescription Pharmacy CRC Vials-Amber in 30s or 90s for one month or three months supplies; for the worst scenario for 90 units DP (Tablet or capsule) dosage X number of such numbers of opening and closing simulating in that prevailing environmental condition at home in a medicine cabinet most likely within the vicinity of the bath-room where there is possibility of high-humidity and in winter temperature conditions. Do all analytics including, assay, dissolution and impurity to find if the last dosage has maintained these quality integrity.
I just wanted to share my own experience and related concern, of going through the pharmaceutical packaging and dispensing evolution which I have come across in my life and over these 50 years being in the US and the practice of DP dispensing and taking of medicine by ultimate user, the patient.





